Transcribed from 0:52–24:13 of the Week 8 recording at lgo.idaho.gov/capitol-clarity/#week-8.
A "bootleg recording", with far clearer audio quality, is available at bitchute.com/video/hfzL5gUeQvxr.
My transcription effort is not complete; the source material was given orally, and thus did not come with a bibliography. I intend to find and insert all cited studies as inline links.
Introduction
Dr. Ryan Cole: I'm Dr. Ryan Cole; I run Cole Diagnostics; it's one of the largest independent laboratories in the state of Idaho; I started it 17 years ago. I'm a Mayo Clinic trained, Board certified pathologist, Board certified in anatomic and clinical pathology—so, yes, I have expertise in immunology and virology—I also have some specialty expertise in skin pathology, so I do a lot of skin cancer diagnostics as well. I've seen about 350,000 patients in my career; we've done about 100,000 COVID tests in the past year, and so it is right up my alley, and so I'm not just blowing smoke today; this is my area of expertise. I want to be able to share with you today actual science. We get a lot of politics from one side, or the other side; I'm not here to offend one side or the other; I'm here to speak data. And the data speaks the truth. And so I have no agenda; I just want people to understand what public health messages have we been missing—what treatments should be available to everybody—we want to talk a little bit about the "vaccines", and then I want to open it up to questions, 'cause I could talk on this for probably 3 hours or 3 weeks. So, you know… I've only read maybe 6 thousand articles in the last year; I've only seen, you know, like I said, 100 thousand patients, so… buckle up, and [hopefully I'll share] something useful… if one person walks away and I help save a life, then I've accomplished my purpose here today, so, thank you for the opportunity… and thanks to [the] Lt. Governor's Office as well [for inviting me to speak]; I'm honored to be here.
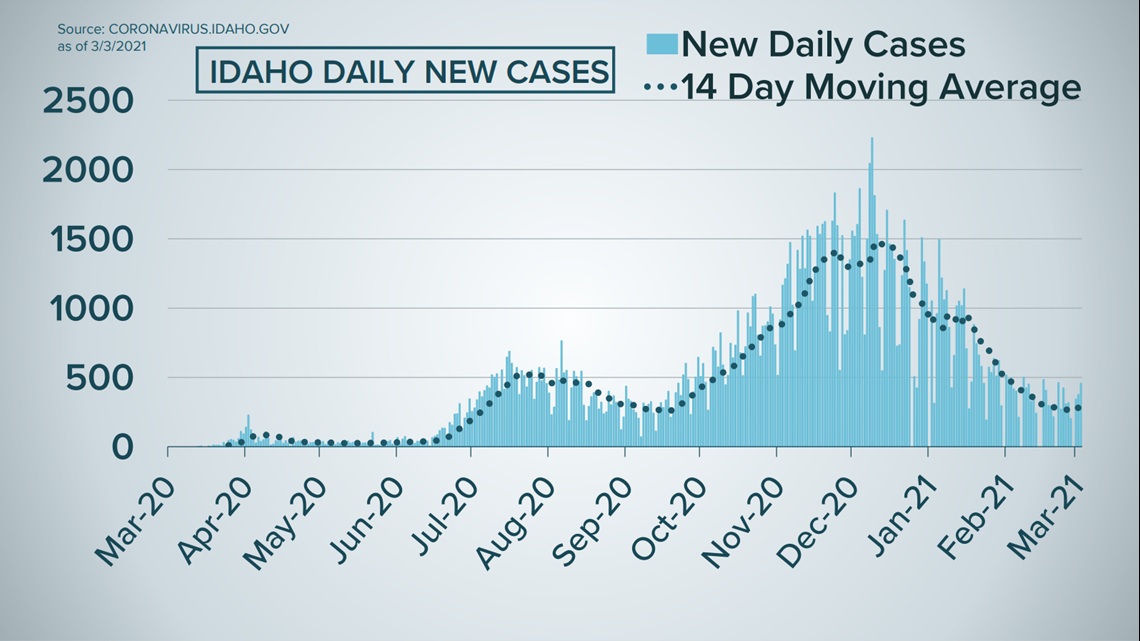
RC: This is where we are right now. Does that look like a pandemic? It was; it's not anymore. We are in an endemic, now. Statistically, the pandemic is over, in Idaho. Statistically, once we're below a set percentage… we are not in a pandemic right now. Is the disease present? Sure, it is. Is it widespread? No. You know, we're still doing, maybe, 500–600 patient tests a day. At most, we're seeing 2% per day right now. And so, the numbers are going way down.
RC: We are past a pandemic stage; we are in an endemic stage—in most states, we are; numbers are still high in a few states—but we're getting past that point, and here's why: coronaviruses are seasonal; they follow a 6–9-month lifecycle, and no matter what we do, they're gonna do what they do, and then they're gonna fade. What happened to SARS? What happened to MERS? What did we do to stop them? Nothing. They did their thing.
RC: Average COVID-19 death age? 78.6yo. Average age of death in North America every year? 78.6yo. That's fascinating.
RC: What are our highest risk factors? Obesity; low vitamin D levels; advanced age. 90% of deaths in [Idaho] have been over 70 years of age. That's the at-risk population. We have stopped our society for something that's taking people that are already at that death-risk age anyway.
RC: The virus is fragile; it doesn't live outside. UV light fractionates it, kills it, blows it apart. Ventilation—the wind—blows it away. It is insanity to wear a mask outside. It is absolute insanity. And that's science: there is not one study that has shown any superspreader event to have occurred outside; they have all been indoors, with poor ventilation.
Vitamin D
RC: [The] biggest lost message on this entire pandemic is vitamin D. …If I could give you all one message to all of you, for every winter and autumn for the rest of your lives, there is no such thing as "flu and cold season". There is only "low vitamin D season". Vitamin D: every cell in your body, every nucleus has a receptor for vitamin D on it. 2,000 genes in your body are controlled by vitamin D—5% of your body's genome, controlled by vitamin D—It is the master key to your immune system… if one has a [vitamin D] level in mid range [50ng/ml, range 20–100], you cannot develop a cytokine storm. Data shows: what kills people? Cytokine storm. If you are in mid-level range, you will not die from COVID, because you cannot get a cytokine storm.
RC: So, we don't just have a viral pandemic; we have an international vitamin D deficiency pandemic. i.e. 70% of the world is immune-suppressed. 70–80% of all Americans are immune-suppressed because they are D deficient. 82–88% of nursing home patients are D deficient. Who's dying at the highest rate? Nursing home patients. 83% of African Americans, 70% of Latinos, 72% of Native Americans, 47% of Caucasians, [are D] deficient. (Well, 70% of Caucasians are [D] insufficient.) 80% of all hospitalized patients, statistically, are vitamin D deficient. 96% of people in the ICU are vitamin D deficient. If you are D deficient, you are immune suppressed; you are susceptible to: the common cold, the flu, coronavirus of any sort, bacterial pneumonia, etc etc etc. The best mask of all is a healthy immune system, and a healthy immune system does not occur if you don't have D in normal range. Well, how do we get D? Sunshine. You know, we synthesize it through our skin. Above the 35th parallel, or below the 35th parallel, for 4–5 months of the year, you cannot synthesize vitamin D through your skin. The older you get, the harder it becomes, as well. Vitamin D is critical. Every Idahoan: if you do not supplement, you are vitamin D deficient; you are immune suppressed (in the fall and winter). …Anybody [in the US living north of AZ, NM, OK, AK, TN, or VA] is vitamin D deficient, all winter long. So, you can run outside, naked, thinking you're getting sunshine, from October through March, like this fine gentleman here in the snow, and the amount of vitamin D you will synthesize, from Oct–Mar, outdoors, running naked in your tutu, [if you live above the 37th parallel,] is zero. Absolutely zero. If you do not supplement with vitamin D in the wintertime, you are immune suppressed.
RC: Most insurance companies in Idaho and northern states do not pay for a vitamin D test, unfortunately. Other countries, Scandinavia, test their citizens twice a year; they supplement 35 foods on their food shelves with vitamin D. Why [are] Finland, Norway, Sweden doing so well? They take care of the public health of their individuals. They know that this is public health message #1 for their immune health, so they do something about it. 80% of Americans also are Magnesium deficient; our soils are depleted. Vitamin D and Magnesium play a fine dance: you need them both to work together in order to have a functional immune system. We're also Zinc deficient, 70–80% of us in this room. Diet, diet, diet, diet: what you eat matters. It affects your immune health.
RC: Obesity drastically reduces your ability to get vitamin D into your circulation. D is a fat-soluble vitamin; the heavier-set you are, the more it goes into your fat and not into your circulation, to stimulate your immune system. Normal D levels also decrease colon cancer, breast cancer, thyroid cancer rates, depression rates, suicide rates. 8 out of the 10 highest suicide states are northern-tiered states, go figure. Vitamin D, it's not a vitamin; it's a prohormone. And, again, it affects thousands of genes in your body. [If] you get a D level up to normal, you decrease risk for all these things, not just COVID.
RC: Most physicians, unfortunately, don't know how critical this is. This should be [the] public health message from the pulpits of Washington, the pulpits of every state. We're pulling our hair, Henny Penny, "the sky is falling, oh no…"; what really matters is: if you have a healthy immune system, you have a healthy population. And we are not emphasizing that. It's "oh gosh, mask, distance, there's nothing we can do…", etc. There is something we can do: give the right message. And the right message is: you can take control of your immune health; you can do something about it. What goes into your body does matter. Public health officials have ignored this critical message. Normal D levels decrease your COVID symptom severity and risk for hospitalization 90%. That's the world data now, there have been a lot of placebo-controlled trials that show this, all around the world. It is scientific fact, not just a correlation like a lot of doctors will say "oh my gosh, that's that vitamin stuff 🙄", and I'm like, no: it's an essential part of the human body. It is an essential prohormone that your body naturally makes in the sunshine, from spring through summer (only a couple hours a day; we can get into that later if there's questions), 'cause there's only about a 3 hour window a day—without your sunscreen (don't tell all of the dermatologists that I serve)—you need to be outside for 20–30 minutes during the spring and summer to get natural vitamin D, and in the fall and the winter you need to supplement to boost your immune system.
RC: The darker your skin, the further north you live, the harder it is to synthesize vitamin D. That's why the hospitalization and the death rates in the darker skinned populations… it is not social disparity; it is plain and simple biology: the darker your skin, the further north you live, the lower your vitamin D level, the higher your risk for COVID and all other illnesses. So, you know, I understand there are some social disparities in our society, and we can't fix that right away (but I hope we're working on it), but the biology of the disease is: the darker your skin, the further from the equator you live, the less vitamin D you synthesize, the more immune suppressed you are. The RDA that was [established] after WWII to sustain basic life, the amount that they give there is like… a drop of water in the ocean, that they recommend. It is nonsense, absolute nonsense. There's a cool app, it's called dminder, and it shows you when you can synthesize your vitamin D.
RC: So, our esteemed Dr. Fauci said in an interview in November, "I take 8,000–9,000 units of vitamin D a day in the winter" [note: I wasn't able to source this claim, though he does take 6,000 IU generally and winter does exacerbate vitamin D deficiency –Ed.], yet, inexplicably, that's not a public health message. In a little side interview [with him], I'd said "you know it affects your immune health; you work for the government and have been in there for 40 years; make that a message to everybody, please".
RC: So, what should public health message #1, #2, and #3 be? Vitamin D; Vitamin D; and Vitamin D. [Also,] decrease societal obesity: cut out the sugar; cut out the processed foods; cut out the carbohydrates. Those are all inflammatory; the more inflamed you are going into an illness, the worse you will do. Obesity is a predisposed inflammatory state; if you are obese, you are inflamed. (I don't say that to offend anybody, but I lost 45 pounds 8 years ago, have kept it off… ask me later about that.) But it contributes to countless diseases.
Red Tape
RC: Is there a treatment for outpatient COVID? Unfortunately, the 3-letter federal government agencies have practiced "therapeutic nihilism", apathy, complete apathy: "if you get sick, go home; if your lips turn blue, then go to the hospital. You can't breathe, go to the hospital." When, in the history of medicine, have we said "well, gosh, you have pneumonia… but, once you're sick enough to be hospitalized and in the ICU, we'll give you an antibiotic for your pneumonia". Insanity… But we, as physicians, have, collectively, lost our medical minds, to say "well, gosh, yeah, you have an illness that we know is killing people around the world; why don't you just go home, and see how you do?" Insanity. The earlier you treat, the more complications you can decrease down the road. And you know what? There's a treatment.
RC: Unfortunately, if there's a treatment for a disease, the federal government cannot approve a vaccine. By law [21 USC §360bbb–3(c)(3)]… So, the NIH, who is involved in approving medications, they co-hold the patent on the "vaccine" with Moderna. If the "fox is not guarding the henhouse" there, I don't know who is. That, also, is insanity, to have the government in bed with a private company, vending a product that they want to give to everybody. And so, when they look at the potential "therapeutics"—hydroxychloroquine, I'm not going to talk about, because [it's] pretty controversial (I have my opinions; I took it for 10 months; I swabbed thousands of sick people; I never got COVID… so, that's my story on that one)—there's a better medication; I'm going to discuss that next.
RC: Conflict of interest: federal government, in bed with a vaccine company. Absolute conflict. They don't want a therapy to work, because then they couldn't vend their vaccine. However, they've tried remdesivir. 6 months ago, the World Health Organization said "stop using remdesivir; it does not add survival rate to anybody". $3,000 a pop, what are our hospitals still doing? Giving remdesivir. When does remdesivir work? The first 2–3 days of disease, when the virus is replicating. By the time you're hospitalized, you are in the hyper-immune phase of the disease; your immune system is what the hospital is trying to tune down. Remdesivir, it's like peeing on a forest fire: it does nothing at that point, because the virus is already maximally replicated. Remdesivir: expensive; of benefit to the pharmaceutical companies and their back pocket; of no benefit to your health. Convalescent plasma: when does it work? The first 2–3 days of disease, when the virus is replicating. Do people get that outpatient? No, they don't; they only get it in the hospital, when it's not effective. Monoclonal antibodies: when do those work? The first couple days of disease, when the virus is replicating. By the time you're in the hospital, when the virus has reached maximal replication, does it work? No, it doesn't. Do steroids work? To a degree, they do: once you're at an inflammatory stage, in the hospital, yes.
Ivermectin
RC: Enter an effective prevention and treatment: Ivermectin!
RC: So, I know a lot of you may [be familiar with this drug already:] we're in farm country, horse country; you give it to your dogs, your cats, your horses; it's an antiparasitic. But, it's a molecule. It doesn't read the textbook and say "I can only kill parasites"; it's a molecule. And, fascinatingly, it works against viruses, too: not just SARS-coronavirus, but a bunch of other viruses, as well. So, in August last year, we found out that it killed [off] coronavirus [by] 99.9% in petri dish studies. The NIH, what did they do? For reasons I already explained, they recommended against it. And they did it on monkey cells instead of human lung cells, [saying] "oh, the dose would have to be too high…" they fudged the data. Unfortunately, it works. It works. So, what did the rest of the world do while we said "everybody go home, let your lips turn blue, then come to the hospital"? The rest of the world said "well, let's try it!"
RC: So, what did the rest of the world do? A lot of trials. [More than 2.5] billion people on the planet have taken this medication since the 1980s. This medication won the Nobel Prize for the discoverer. It is that safe. It is on the world's safest and most essential drugs list. [More than 2.5] billion people have taken it, with only 1 or 2 deaths out of [that], and those people had a genetic disorder. Super, super, super safe. We've given it to people [at] 30 to 40 times the recommended dose: no adverse effect. In the world studies—and again, therapeutic nihilism, here: we're finally just starting to do some studies—some brave doctors from Texas and Florida and Wisconsin have been using it in their hospitals; they have decreased their death rates by 70–90%, in their hospitals. 70–90. In Houston, one hospital was using it; now, all the hospitals in Houston are using it, because they saw what the one brave doctor was doing.
RC: It is an approved medication; it is safe. Is it off-label? Yes. Is the FDA approving it [for the treatment or prevention of COVID-19] yet? No. Because the smart doctors around the world "aren't smart enough; only American doctors are smart; we have to do the trials here." Meanwhile, Pfizer got their approval from studies overseas, not done here, so it's absolutely hypocritical of our 3-letter agencies to be approving certain things that were done overseas, and then not approving things that were done overseas… Placebo-controlled trials, there are 15,000+ patients, in meta-analysis… no matter what your therapy is, Ivermectin, if that's added to the mix, it decreases the death rate by 75%; if given early, by 85%. What does that mean? Of the half-million deaths we have in North America, we would have 375,000 [fewer] deaths. There is blood on the hands of bureaucrats in Washington who have suppressed this life-saving medication. Blood on the hands of those individuals. How much does it cost? $0.02. In India, an entire province—200 million people—COVID's gone. They put little blister packs together for $0.02, gave it out to their entire population… they're at their grocery stores; they're at their theaters; they're walking around; they're living normal life. Wherever it has been given in the world, they're back to normal life. In the U.S., it's compounded for about $2–$5 per dose; you can get a full course of treatment for under $30. And decrease the death rate by 75–86%.
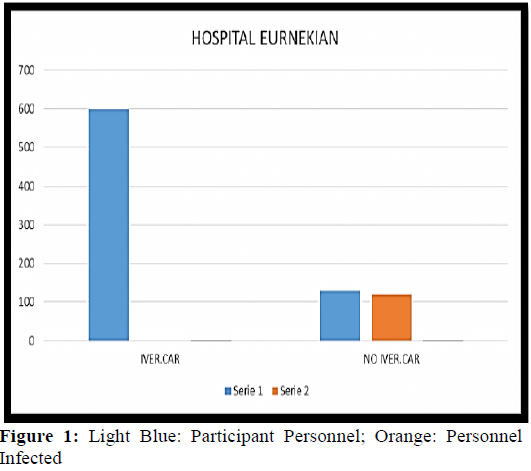
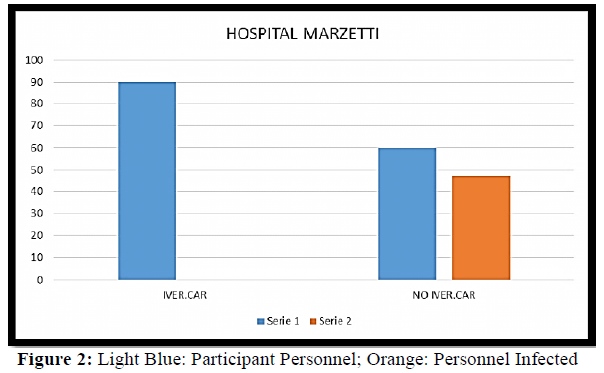
RC: So, finally, some of the data from the world was presented, and the NIH hemmed and hawwed; they only looked at 11 studies, instead of the tens and tens and tens and tens of other studies; and they said "ah- there's one that shows maybe no benefit"… 100% of the world trials have shown benefit. It decreases acquisition—prophylactically, I've been on it for 2 months now—in Argentina, in a hospital trial, it prevented 100% of acquisition in healthcare workers. 800 doctors and nurses were given it, during their big outbreak; of the 800, 0 got COVID; placebo group, 57% got COVID, that were not on ivermectin.
RC: Scandinavian studies: prevented acquisition by 88%.
RC: Multiple mechanisms of action of this molecule—don't have time, long medical lecture, but it's fun to know—the beauty of it: it can cover all the variants, because of its mechanisms. All the variants. Unlike, "oh, we're going to have to give you a new formulation of this vaccine or that vaccine or that vaccine…" No! The mechanisms of action of this molecule against this virus don't stop.
RC: There's a great [organization, FLCCC], these are the doctors that are front-line, pushing this forward, and they're the ones that got the NIH to finally listen, to finally take a neutral stance, to un-shackle the hands of the physicians that can prescribe it. I can say that I've saved 42 lives in the last 2 months (I don't prescribe very often; generally, I'm behind the microscope or in the lab, but, you know, from one case to another, and nobody doing anything…)
RC: Elderly, obese, 83yo, 72yo, asthmatic, diabetic… to a T, every person that's had COVID I've treated with this has been better in 12–48 hours. 12–48 hours. To a T.
RC: 42 people. That's a small case series of patients… I know it works.
Vaccines
RC: All right, vaccines—OK, I'm going to be a little controversial here and may frustrate a few people—by definition, a vaccine, historically, is giving a protein or an antigen or a part of a pathogen and/or a whole, killed pathogen. Injecting a sequence of mRNA into a human being is a medical device. Historically, what we're doing right now does not fall under the definition of a "vaccine". They shifted the verbiage in some of the federal register back in October so they could approve this. So, it was a slight of hand to change the verbiage… what we have right now is an experimental biological gene therapy immune modulatory injection. We are injecting people with a synthetic sequence of nucleic acid. We have never done this on a large scale in human history.
RC: mRNA trials in mammals have led to odd cancers; mRNA trials on mammals have led to autoimmune diseases—not right away: 6, 9, 12 months later—So… what we're doing right now are not approved "vaccines"… how do you create demand? You create scarcity. "Oh my gosh, we can't get a shot; we can't get a shot!" Well, it's a beautiful marketing ploy to be able to say "gosh, there's a low supply", so that everybody wants it now. Well, everybody may want it, but, the long-term safety data, it's not there. 50% of healthcare providers are absolutely not getting this injection, and that's the reason: we don't trust the data. The fox guarded the henhouse; the companies did their own data—there were no independent observer groups looking at the data.
RC: Do the shots decrease severity of the disease, and hospitalization [rates]? Well, they seem to be [doing so]. But they don't fall under the definition of creating pure immunity, and preventing transmission. If you're immune after an injection, why in the world would you still have to mask and social-distance? That is an admission that they don't know that it's a vaccine, and that's an absurdity. There's no long-term proven safety.
RC: My biggest concern, honestly, is antibody-dependent enhanced reaction: you get a shot, you're fine, it's preventing this, preventing that… I'm not "anti-vaxx", not "tinfoil hat"; I've had lots of vaccines; my kids have had vaccines; that's fine, but if you get a coronavirus shot—historically: SARS, MERS, animal coronaviruses—you get a shot, when you're exposed to a wild-type variant of the virus 6, 9, 12 months later, [your] immune system can go haywire. In the SARS vaccine trials, in the ferrets and the monkeys, 100% of the animals, when exposed to a wild-type virus, ended up with immune reaction.
Closing
Host: [Inaudible]
RC: I'm sorry; I'm probably going too long, aren't I? I'll just wrap it up. So, the vaccines are an experiment on society. Here's my comment on masks:
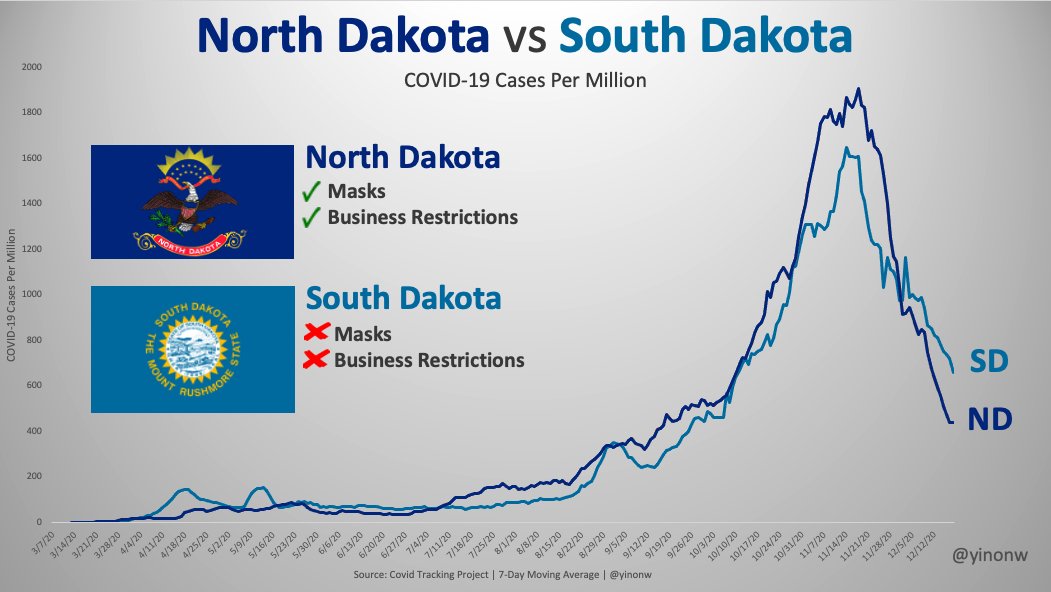
RC: Two states, one with… masks and business restrictions; the esteemed governor Noem, no masks, no business restrictions; there's your curve of coronavirus. You can draw your own conclusion as to whether masks do anything (I can tell you: they do not.)
RC: Conclusions (lots of conclusions here…):
RC: Public health message #1. prohormone/vitamin D, critical to every Idahoan's immune health. That should be public message #1, every fall and winter, every year, for the next hundred years. Absolutely.
RC: #2. There is an outpatient, early, effective prevention and treatment for COVID: Ivermectin.
RC: #3. Your body, your choice; in my opinion, the vaccine is unproven, and the long-term safety is not there. We are at an endemic now; we are not in a pandemic.
RC: That's my $0.02 on coronaviruses, and I thank you for the opportunity…
Q&A
Q: Is ivermectin effective against other viruses?
RC: Yes, it is. It's effective against dengue virus, to a degree; partially effective against ebola virus; it's effective against all coronaviruses; it's effective against certain mechanisms of certain viral families—West Nile included, which hits Idaho.
Q: I've heard that mRNA produces adverse effects on [the] placenta…
RC: Again, long-term safety data isn't out. There are some studies that indicate this type of virus, especially, after you've given the shot, and the mRNA is there, that the spike protein, it's called a syncytial cell, and the placenta is a conglomeration of a bunch of cells… and it can stick to the surfaces of those type of cells; it can cause an immune reaction, and can cause an autoimmune attack. I have a friend whose wife, 7 months pregnant, got the vaccine… just miscarried yesterday, right after the injection.
Q: Can you define "cytokine storm"?
RC: [This was a very visual explanation, which I have adapted for text. I take the blame for any distortions I've introduced to his explanation. –Ed.] in our immune system, we have a lot of white blood cells, certain ones… it's a little "army", fighting off things, and [sending] a signal to this soldier, that soldier… so one soldier sends out this type of cytokine, recruits another white blood cell, another white blood cell, so you have your inflammatory cytokines that ramp up your immune response, and then you have your calming cytokines that calm it down. If you have low vitamin D, all those signals [can form a positive feedback loop of inflammatory cytokines leading to] death; if you have adequate vitamin D levels, all those genes turn on and off [to appropriately signal positive and negative feedback in a control loop]. So, cytokines are just signals "from one soldier to another" in the battle against a disease; you want a cytokine response to a set degree, but then you want it to go down. How can your body naturally do that? Get your vitamin D level normal, all the genes talk to each other, improves immune health… best mask of all.
Q: Can the lipid nanoparticles in the vaccines cause a cytokine storm?
RC: The lipid nanoparticles in these shots… 70% of us are allergic to polyethylene glycol. (That is antifreeze.) Polyethylene glycol 2000 is one thing that they're putting to keep it from freezing. That can absolutely cause an anaphylactic reaction in a lot of people.
Q: Will we be able to get ivermectin from doctors in Idaho?
RC: A lot of physicians are very guideline-driven, and very… "what's the protocol", "what's the guideline", "what's the word from Washington?" instead of "I have a black bag; I have a medical degree and a license to practice; and I have a thinking brain…" 1 out of 5 medicines in America is written off-label for another disease—it's approved; these are approved medicines—you're just using it for a different condition. The short answer is: if you can't get it from a local doctor, there are online physicians, all around the country, that will prescribe it… there are a bunch of online sites.
RC: I know a handful of brave individuals that are prescribing it, saving lives. It's frustrating to try to get the data to my colleagues, and say "guys, we don't need the degree of death we're seeing", and [that] this is a preventable disease… you can prophylax; you can treat. And, not only that: down the road, if you have long-term symptoms, ivermectin can tune those down, as well. It is a phenomenal medication. And it's an immune modulator, not just a viral killer.